
Diabetic amputations are one of the most preventable and life altering medical procedures, so why is the number of amputations rising in low income communities?
Elena Norwood, a young college athlete in her senior year at a private university, was recently diagnosed with type one diabetes. Elena had felt tired and suffered from headaches most of the fall semester, but so had everyone else. It was her second college semester in a pandemic, with Zoom classes and little to no social opportunities to let loose. She realized something was wrong while she was visiting her family in California during winter break. After a doctors appointment and some routine blood tests, she was instructed to go to the emergency room. She was going into ketoacidosis — a life threatening complication where blood becomes acidic. She remembers dismissing her symptoms over the past few months, her hospitalization coming as a shock. Elena is a close friend of mine, and shared with me that it was a close call for her — she said she was almost dying.
Although her diabetes is now under control, the recent snow storm left her with new health concerns. The storm posed a unique problem for her because she needed to drink water (drinking sodas or other drinks could spike her sugar), and she needed fatty and protein filled foods, which were sold out in most stores around us. My roommate and I brought her water in exchange for some heat and some good laughs with friends, and I saw firsthand how diabetes has upended her daily routine. She is fortunate enough to have a glucose monitor, but she still does a lot of manual finger pricking to make sure her levels are good. Mealtime is a math problem. Elena showed me how she calculates her doses based on the carbohydrates in the foods she is eating and tries to dose her insulin the best she can. In addition to dosing during meal times, she also has to take a long acting insulin everyday. Elena elaborated that it was frustrating to pay extortionist prices to manage her care and accused companies of maximizing their profits by putting unnecessary time locks on glucose monitors.
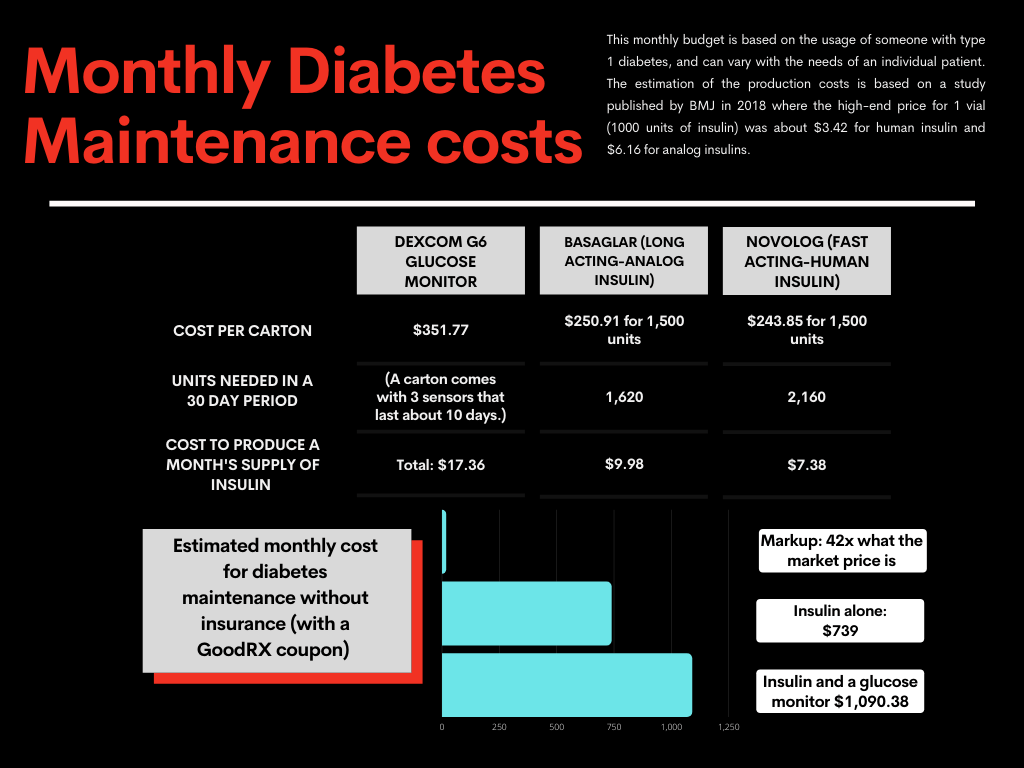
Healthcare companies unabashedly treat diabetes care like big business. Nick Jonas recently came under fire for promoting the ease of a glucose monitor in a five million dollar ad while many diabetics risk infection to extend the life of theirs. This five million dollar ad could have provided a year’s worth of life saving insulin for 20,000 people. Allowing the healthcare industry to operate for profit quite literally gives them free reign to put a price on people’s lives, and stick taxpayers with the bill. The mark-up on insulin causes many diabetics to ration, a choice that can have fatal or near-fatal consequences. People needlessly die because they don’t have access to a medication that costs $17 to produce. Chronic diseases like diabetes are cash cows for pharmaceutical companies, and minority communities are often hit hardest by the inexorable costs of preventative care and management.
The Racial Disparities of Diabetes Care and Management
In a May 2020 article published by ProPublica, a startling pair of maps illustrate a grim reality: a correlation between enslavement in the 1860s and the rate of diabetic amputations from 2007-2009. The article details the efforts of Foluso Fakorede, an African American doctor, to help these patients who are often overlooked by the healthcare system. The U.S healthcare system regularly cuts spending on preventative care and leaves low income patients to develop even more life-threatening and costly complications. The people affected are invariably the underprivileged, a precarious position in the U.S. healthcare system, which has only been further destabilized by the Covid-19 crisis. The maps I mentioned earlier show striking similarities in the Mississippi Delta and the Rio Grande Valley. Like the Mississippi Delta, 50% of the Rio Grande Valley is considered a food desert, defined as an area where residents have to go more than 10 miles to reach fresh food. The increase in diabetic amputations, a highly preventable and life altering surgery, is a harrowing reminder of the racial divide in our healthcare system.
At every turn, poverty and race complicate an already dire situation for most people. While people of color are far more likely to develop diabetes and experience complications, this is a reflection of a history of marginalization, not genetics. Lifestyle changes that successfully prevent or mitigate the life altering effects of diabetes are not viable for impoverished people working long hours for little pay. Lack of access to fresh and nutritious food compounds the risk of diabetes, and leaves little chance for people to successfully manage their diabetes even if they get diagnosed. Healthy food is expensive in the best of times, and when people are already experiencing food insecurity at startling rates, they’re more likely to take what they can get. Low income communities are often over policed, and may not be able to exercise outside as easily because it poses unique risks. Dr. Donald Warne, president of the American Indian Health Management and Police argues that there is a “direct biochemical connection between living in poverty and the stress that people are under and blood sugar control.” Even the depression that many diabetics experience is amplified by socioeconomic factors. The nerve damage that often comes along with diabetic complications means that some patients don’t even notice the sores and blisters until they have gotten progressively worse. When patients finally get treatment, their amputations require extensive aftercare and most cannot take time off work to let it heal, only leading to further infections and emergency room visits.
The Texan Diabetes Crisis: lessons from the southern border
In the Rio Grande Valley the diabetes epidemic is particularly acute with a higher incidence than other large Hispanic communities in Texas like Houston and San Antonio. The number of amputations is 50% higher than the state average. Even though most amputations could be avoided together by proper management and preventative healthcare, access to these resources is scarce. Daniel Zamora, a resident of the Valley whose parents died from diabetes, didn’t even have healthcare coverage until his condition had already progressed severely. Zamora would go to the ER when the situation was really dire, but until then he would try to self medicate with traditional medicine or rubbing alcohol.
Zamora’s story is unfortunately a common tale for residents of the Rio Grande Valley. A study published in 2019 by UT Health San Antonio found that despite nationwide declines in amputations, they had remained stable in Texas. They found that Hispanic communities like Zamora’s were more vulnerable to lower extremity amputations because of the barriers of regional poverty, especially among the uninsured. Lack of medical resources leaves patients like Zamora with a hard choice. They can spend what little they earn from working to go to a doctor, most likely missing work in the process, or ignore it and focus on more pressing life challenges such as getting enough food on the table or taking care of other family members. Poverty often forces people to put personal health on the back burner.
Residents of the Rio Grande Valley experience a healthcare system that is severely overburdened and underfunded. Because so many have to navigate without insurance or preventative care they often avoid seeking medical treatment until situations are dire. Most residents don’t have regular patient-doctor relationships, as many can’t consistently afford to see healthcare providers and thus rarely form lasting relationships with them. Even those that do have Medicare and Medicaid still experience a different level of care from those with privatized insurance. A 2019 study found that while revascularization was associated with less amputations, the procedures were generally not done for patients with Medicare and Medicaid.
The future of Diabetes in the Rio Grande Valley
The rate of diabetic amputations is only likely to get worse, with experts predicting that the number of adults diagnosed with diabetes will triple by 2060. In the Rio Grande Valley alone, health experts believe that almost one-third of the population is diabetic.
Many people believe that education and preventative programs like community blood sugar level testing can help address the epidemic, but without a real restructuring of the broader healthcare system, this is just a stop gap. Nonprofits like Salud y Vida and Proyecto Juan Diego offer a great resource to the community, but they can’t give residents of the Valley the income to afford nutritious foods or the healthcare providers they need to see to manage their condition. But it doesn’t have to be this way: a year’s supply of insulin should cost about $130. Over 30% of Rio Grande Valley residents live below the poverty line, and most would never be able to afford $1,000 a month to manage their symptoms. For people who are already struggling to balance working and caregiving in addition to living and food costs, this is an unimaginable task.
The sum of diabetic complications costs the healthcare system more than properly preventing and managing diabetes. There is an economic domino effect on communities by taking breadwinners out of the workforce while they care for family members. These hardships are in large part preventable through education and healthcare reform. No one wins in the current system — diabetes can affect anyone, even if they maintain a healthy diet and lifestyle. Unfortunately, it also hits already vulnerable communities the hardest, and exposes the ever widening gap between healthcare, race, and poverty in the U.S. We need an overhaul in terms of our healthcare system to rebalance the scales and put individuals over profits. This begins with preventative care in the most vulnerable communities like the Rio Grande Valley, but medicine price ceilings and universal healthcare would address the root of the problem in our society.
Categories: Texas
